Use an evidence-based clinical pathway to guide screening and management of suicide risk
Evidence-based clinical pathways give guidance on how to manage patients who screen positive for suicide risk. Having a detailed process in place will save time and resources when responding to a positive screen. The pathway below provides an overview of a suicide prevention strategy. Please see the text that follows for more detailed descriptions of each step.
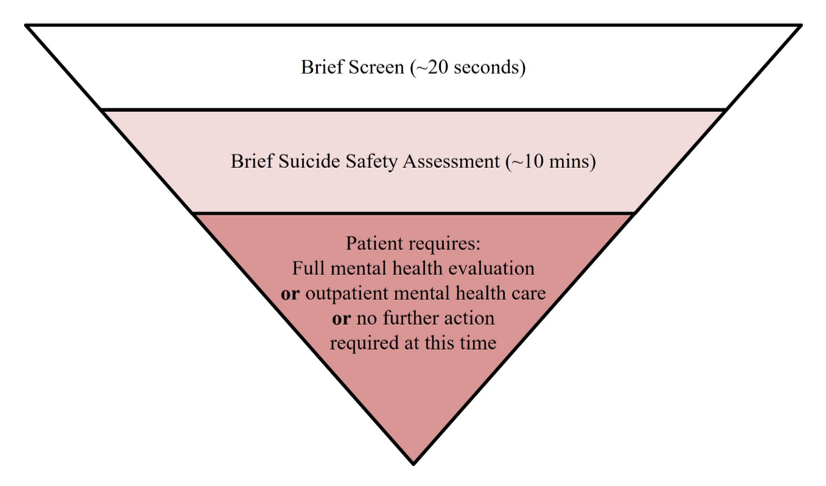
Source: NIMH ASQ Toolkit
Consider this 3-tiered youth suicide risk clinical pathway developed by an American Academy of Child and Adolescent Psychiatry (AACAP) Pathways to Clinical Care suicide risk workgroup for the inpatient and ED setting (available here), and NIMH adapted the pathway for the outpatient and specialty care settings (available here). It has 3 main steps (as mentioned in the above diagram):
Brief Screen (less than a minute)
Screening is a way to identify someone who needs further mental health evaluation. There are no suicide risk screening tools that can predict who will die by suicide; therefore, anyone who screens positive on a screener needs further evaluation.
- Screen all patients ages 12+ years for suicide risk during preventive service visits, using a validated suicide risk screening tool
- Screening can be included with other adolescent intake screeners. If the patient screens positive, a portion of the well visit may need to be postponed. This would be akin to finding a physical ailment on routine exam that then takes precedent over the well visit
- For youth aged 8-11 years, targeted screening strategies may be implemented for patients presenting with behavioral health symptoms
- Youth below the age of 8 years should not be screened for suicide risk, as it is unclear if children at this age can comprehend the screening questions on existing tools
- Clinicians can assess for suicide risk in young children when a parent reports suicidal behavior, or when patient presents with depressed mood, severe irritability, or suicidal ideation or history of suicidal behaviors
- For detailed information, see Screening for Suicide Risk in Clinical Practice.
Brief Suicide Safety Assessment (10-15 minutes)
This step is different from the screen, which simply identifies risk. The assessment is a conversation with the patient that assists in further triage by evaluating the frequency of suicidal thoughts, plans, mental health symptoms, suicide history, supports, and other factors. This is the most critical step of the pathway because it identifies appropriate safety needs and guides next steps for the patient.
- This should not be a full mental health evaluation but rather a brief way for clinicians to decide what the patient needs next
- A brief suicide safety assessment can be conducted by a physician, social worker, nurse practitioner, physician assistant, or other mental health professional. These individuals should have advanced training and be trained to administer a brief suicide safety assessment
- There are tools that can be used to guide a clinician in conducting a brief suicide safety assessment
- For detailed information, see Conducting a Brief Suicide Safety Assessment.
Disposition: Identify next steps for care, based on the brief suicide safety assessment
Imminent Risk: Patient requires an emergency mental health evaluation
- The patient has acute suicidal thoughts and needs an emergent full mental health evaluation
- If there is not an onsite mental health professional embedded in the practice, send the patient to the emergency department (ED) or engage a mobile crisis team or acute mental health evaluation center for extensive mental health evaluation (unless contact with a patient’s current mental health provider is possible and an alternative safety plan for imminent risk has previously been established)
- For detailed information, see Caring for Patients at Imminent Risk of Suicide.
Note: It is rare for patients presenting to a medical setting with medical chief complaints to be at imminent risk for suicide. However, your clinic should have a plan in place for how to manage patients who require urgent evaluation (see section on caring for patients at imminent risk of suicide).
Further Evaluation is Needed: This is not an emergency, but patient will require further mental health evaluation from a mental health professional as soon as possible.
- The patient is non-acute positive and is not at imminent risk for suicide but remains a moderate risk and needs a full mental health evaluation from a mental health professional or a primary care provider with sufficient training in the assessment and management of mental health conditions
- If mental health evaluation is not available within your practice, refer the patient to an outpatient mental health clinician for the full evaluation
- Take steps to protect the patient’s safety for when they go home
- For full details, see Caring for Patients Who Need Further Mental Health Evaluation.
Low Risk: No further evaluation is needed at this time.
- Determine if the patient might benefit from non-urgent mental health follow-up
- Send patient home with a mental health referral if indicated
- For full details, see Caring for Patients at Low Risk of Suicide.
Last Updated
02/22/2023
Source
American Academy of Pediatrics