Many individuals with prenatal alcohol exposure (PAE) who are seen in pediatric practices manifest developmental and behavioral challenges. Differential diagnoses for an individual with PAE can involve additional testing to determine growth deficits and dysmorphic facial features related to other syndromes, and to identify co-occurring conditions.
Differential Diagnosis: Growth Defects and Dysmorphic Features
Many individuals with prenatal alcohol exposure (PAE) who are seen in pediatric practices manifest developmental and behavioral challenges. Differential diagnoses for an individual with PAE can involve additional testing to determine growth deficits and dysmorphic facial features related to other syndromes, and to identify co-occurring conditions.
Differential diagnoses for an individual with prenatal alcohol exposure can involve additional testing to determine growth deficits and dysmorphic facial features related to other syndromes. These features are present in less than 20% of children with an FASD.
Differential diagnoses of growth deficits in individuals with prenatal alcohol exposure
Some individuals with prenatal alcohol exposure can have growth deficits in height, weight, and head circumference at some point in development, including being small for gestational age. However, these growth problems may be in the mild range and above cutoffs for microcephaly or short stature and may not be prominent at birth. This requires pediatric developmental surveillance and monitoring. Reviewing nutrition to ensure adequate caloric and nutrient intake is an important part of such surveillance and monitoring.
There are many causes for growth deficits in individuals, including environmental, endocrine and/or genetic factors. Referral to a pediatric endocrinologist or pediatric geneticist may be in order because of the complexity of this differential diagnosis.
Some of the most common syndromes/conditions associated with growth deficits may include but are not limited to:
- Turner’s Syndrome
- SHOX Gene Haploinsufficiency
- Idiopathic Short Stature
- Growth hormone (GH) deficiency
- Chromosomal defects
- Chronic illness
- Dysmorphic features
- Low birth weight
Differential diagnoses of dysmorphic facial features that could be consistent with prenatal alcohol exposure
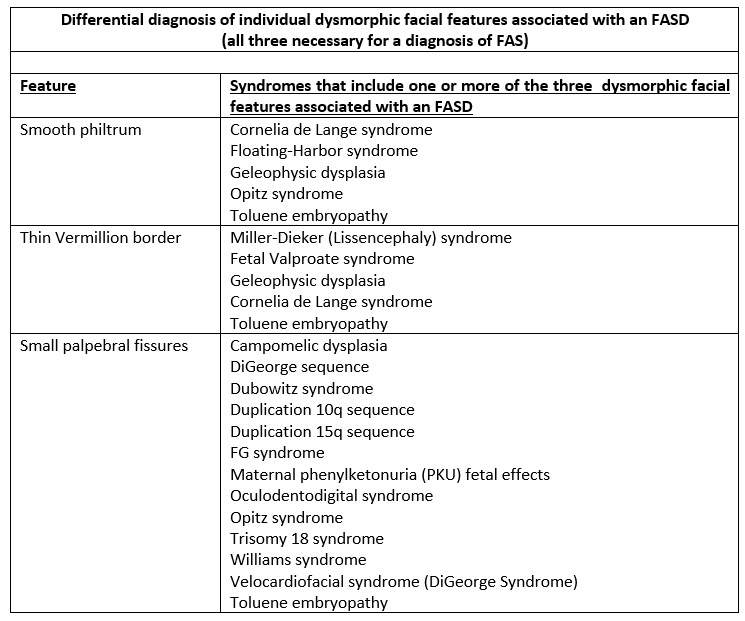
Some individuals with prenatal alcohol exposure and an FASD have a constellation of distinctive dysmorphic facial features: small palpebral fissures, smooth philtrum, and thin upper lip/vermillion border. All three of these cardinal features are required for a diagnosis of Fetal Alcohol Syndrome but may be present in other FASDs. View the resource, “Dysmorphic Facial Features of FASD” for a detailed description and visuals of these features.
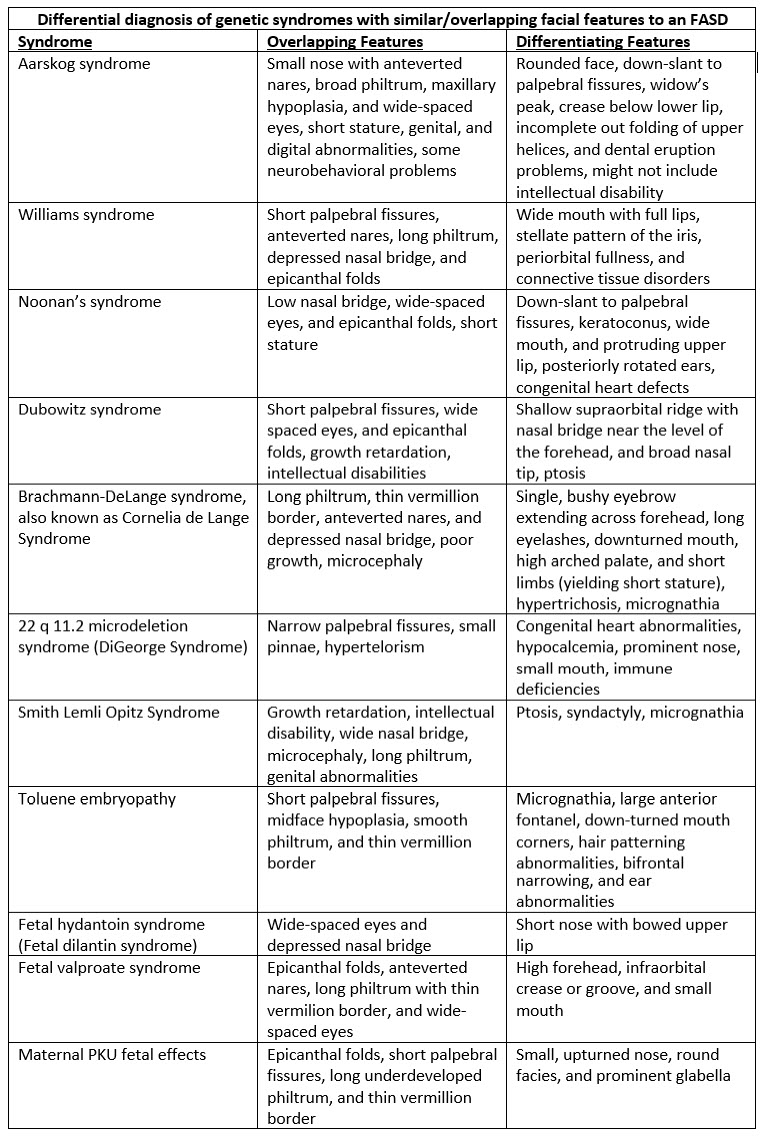
There can be an overlap of dysmorphic facial features seen in prenatal alcohol exposure with other syndromes causing dysmorphic facial features. Other factors concerning dysmorphic facial features include:
- Individual dysmorphic features are not unique to any particular syndrome.
- There are some syndromes in which the constellation of features (primary, occasional features, or both) gives a presentation similar to the presentation of a child with prenatal alcohol exposure. These syndromes should be considered in particular when completing a differential diagnosis.
- In addition to the three cardinal dysmorphic features, children with prenatal alcohol exposure may have additional minor physical anomalies (for example, ear anomalies, micrognathia, or anteverted nares).
View the table of genetic syndromes with overlapping and differentiating features to an FASD.
View a list of syndromes and conditions with dysmorphic facial features that overlap with prenatal alcohol exposure.
Evaluating growth deficits and dysmorphic features
When a pediatrician considers prenatal alcohol exposure as a cause for growth deficits or dysmorphic facial features, other factors need to be ruled out. Additional considerations include:
- Screen for prenatal alcohol exposure as a diagnostic basis for growth deficits at all stages of development (including birth) and/or dysmorphic features related to an FASD.
- Conduct developmental surveillance and monitoring or refer to endocrinology or genetics as indicated.
- When possible, work with a geneticist to identify the appropriate combination of genetic testing, microarrays, and/or Fragile X testing to diagnose genetic disorders that result in specific growth deficiencies (for example, dwarfism and bone dysplasia).
- Remember genetic syndromes and diagnoses such as autism and ADHD can be co-occurring conditions with an FASD.
Additional Resources
Co-occurring Conditions
Growth Deficits
Last Updated
12/11/2023
Source
American Academy of Pediatrics