Early assessment and diagnosis of an FASD can reduce the risk, incidence, and impact of secondary as well as co-occurring conditions such as learning disabilities, mental illness, substance use disorder, school failure, social deficits, and interactions with the criminal justice system.
Appropriate and early access to evidence-informed interventions can favorably impact some of the common challenges experienced by children with FASDs and their families, including speech and language development, executive functions, academic skills, visual motor integration, fine motor coordination, and behavioral issues.
FASD Assessment Areas
The clinical presentation of individuals with FASDs varies in symptom range and severity. This variability in presentation results in part from differences in the quantity and timing of alcohol consumption, the pattern of prenatal alcohol exposure (i.e., chronic or binge exposure), individual genetic differences, and postnatal experiences including but not limited to socioeconomic factors, educational opportunities, and parenting style.
To assess an individual for a potential FASD, one must explore a history of prenatal alcohol exposure; occurrence of developmental, cognitive, and/or behavioral concerns; presence of dysmorphic facial features and/or physical anomalies; and existence of any prenatal or postnatal growth deficits.
Trauma Informed Approach
A child’s adaptation to a stressful environment may result in dysfunctional behaviors and in risks to future health. Physician awareness of an individual’s past and ongoing trauma is important to the assessment and to the differential diagnosis of an FASD. It can be difficult to distinguish the ongoing effects of trauma adaptations from the behavior seen with ND-PAE. Both are associated with poor executive function, cognitive challenges, and emotional instability. Unfortunately, toxic prenatal exposures and postnatal toxic stress often coexist. When they do, a pre-existing neurodevelopmental condition like ND-PAE may impair a child’s resilience in the face of trauma/toxic stress and magnify adverse consequences.
Assessment for an FASD
Monitoring growth and head circumference are also a routine part of health supervision. Measurements of growth deficiency below the 10th percentile [insert and anchor pp 2-5 can trigger a closer look at prenatal alcohol exposure history and development. Screening for facial features is a simple addition to the physical exam. Standards can be found here and cards for use in clinic can be ordered here.
Refer and follow up if the child demonstrates cardinal dysmorphic facial features, prenatal alcohol exposure and/or generalized cognitive deficits and behavioral or global deficits. Most neurobehavioral assessments will require assessment by a psychologist, neuropsychologist or other qualified examiner with sufficient experience.
Any assessment that leads to a diagnosis of an FASD must include a history of prenatal alcohol exposure.
An individual that had prenatal alcohol exposure may be diagnosed under the FASD umbrella, that includes Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure (ND-PAE), Alcohol-Related Neurodevelopmental Disorder (ARND), Fetal Alcohol Syndrome (FAS) and Partial Fetal Alcohol Syndrome (PFAS), and Alcohol-Related Birth Defects (ARBD).
Developmental, cognitive, and behavioral assessment for an FASD
- Neurobehavioral Disorder associated with Prenatal Alcohol Exposure (ND-PAE)
Individuals with neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE) have neurodevelopmental, neurobehavioral, or mental health effects of prenatal alcohol exposure with or without the associated physical dysmorphia. ND-PAE manifests in functional impairments of neurocognition, self-regulation, and adaptive functioning. Although these broad domains overlap with other childhood disorders, specific deficits within them are indicative of ND-PAE.
Impaired neurocognitive functioning as manifested by one or more of the following:
- Global intellectual performance (i.e., IQ of 70 or below, or a standard score of 70 or below on a comprehensive developmental assessment)
- Executive functioning (e.g., poor planning and organization; inflexibility; difficulty with behavioral inhibition)
- Learning (e.g., lower academic achievement than expected for intellectual level; specific learning disability)
- Memory (e.g., problems remembering information learned recently; repeatedly making the same mistakes; difficulty remembering lengthy verbal instructions)
- Visual-spatial reasoning (e.g., disorganized or poorly planned drawings or constructions; problems differentiating left from right)
Impaired self-regulation as manifested by one or more of the following:
- Mood or behavioral regulation (e.g., mood lability; negative affect or irritability; frequent behavioral outbursts)
- Attention (e.g., difficulty shifting attention; difficulty sustaining mental effort)
- Impulse control (e.g., difficulty waiting turn; difficulty complying with rules)
Impaired adaptive functioning as manifested by two or more of the following, one of which must be either a communication deficit or an impairment with social communication and interaction:
- Communication deficit (e.g., delayed acquisition of language; difficulty understanding spoken language)
- Social communication and interaction (e.g., overly friendly with strangers; difficulty reading social cues; difficulty understanding social consequences)
- Daily living skills (e.g., delayed toileting, feeding, or bathing; difficulty managing daily schedule)
- Motor skills (e.g., poor fine motor development; delayed attainment of gross motor milestones or ongoing deficits in gross motor function; deficits in coordination and balance
View information on Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure (ND-PAE) that includes details in ND-PAE Age Dependent Symptom Diagnosis Guidelines and differential diagnosis in Differential Diagnosis for ND-PAE.
Download the Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure training presentation
- Alcohol-Related Neurodevelopmental Disorder (ARND)
Individuals with ARND were prenatally exposed to alcohol and have associated neurodevelopmental and behavioral effects without all of the cardinal dysmorphic features or growth problems of FAS. Specific criteria for a neurodevelopmental impairment include neurocognitive deficits, self-regulation problems, difficulty learning, and adaptive function skills.
As noted above, ND-PAE and ARND are overlapping and similar but with a major difference. ND-PAE can be present with or without dysmorphic features, whereas ARND is without the presence of full cardinal dysmorphic facial features found in individuals with FAS. For a diagnosis of ARND, confirmed prenatal alcohol exposure is necessary. In contrast, ND-PAE requires confirmation of ‘more than minimal exposure’ as outlined in the DSM-5.
The DSM 5 Taskforce reviewed scientific information to bring consensus on clinical criteria on the DSM-5 Diagnosis to Recognize Alcohol-Related Neurodevelopmental Disorder (ARND).
- Additional information on NDPAE and ARND
Recent scientific studies about FASDs focused on the neurocognitive and neurobehavioral presentations of individuals with ND-PAE. Prior to research on ND-PAE, diagnostic schema used the term alcohol-related neurodevelopmental disorder (ARND).
ND-PAE, while based on clinical research, was developed in clinical environments, whereas ARND was developed within research environments.
Assessment and diagnosis of a child with either ND-PAE or ARND are important to help pediatric care providers and parents understand a child’s neurobehavioral strengths and limitations while providing a framework for parents and teachers to employ necessary developmental and educational interventions for the child’s success. It is important to recognize that features of ND-PAE are very similar to those of attention deficit hyperactivity disorder (ADHD), and that ADHD is a commonly found co-occurring condition. When assessing a child for ADHD, always include an assessment of prenatal alcohol exposure, growth parameters, and facial features.
Fetal Alcohol Syndrome (FAS) and Partial Fetal Alcohol Syndrome (PFAS)
To make the diagnosis of FAS, an individual must meet all the following diagnostic criteria:
- Prenatal and/or postnatal growth deficiency (≤ 10th percentile for head circumference, age and gender for height or weight or both); this can be prenatal growth restriction, such as in a child born small for gestational age, or postnatal growth restriction.
- Three (3) specific facial abnormalities:
- Smooth philtrum (the ridge under the nose and above the lip)
- A thin upper lip (referred to as a thin vermillion border)
- Reduced palpebral fissure length (the distance from the inner corner to the outer corner of the eye)
- Any of a range of recognized neurodevelopmental or neurobehavioral conditions.
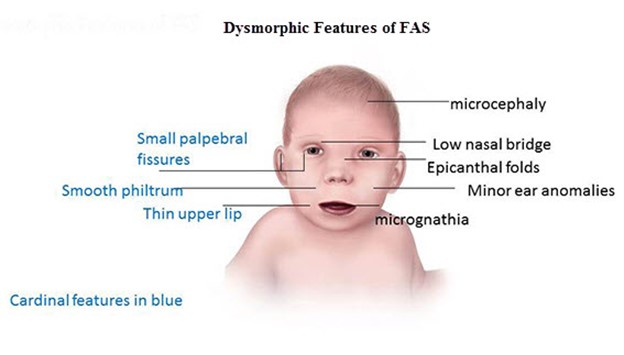
Dysmorphic features change over the life span due to changes in fat deposition, collagen balance, and maturing bone/skull structure. Many of the features of FAS are most evident during the preschool to early school age period.
- While the 3 cardinal facial dysmorphic features are required for a diagnosis of FAS, there are other features that occur with increased frequency in individuals with FASDs and can include:
- Epicanthal folds (small flaps of skin on the inner lower eye lid that cover the inner corner of the eye),
- “Railroad track” ears (outer ears with extra ridge)
- Clinodactyly (fingers that curve away from the thumb)
- “Hockey stick” palm crease (crease has sharp angle toward fingers)
- Low nasal bridge
Lip and Philtrum
The Lip Philtrum Guide is used to rank the upper lip thinness and philtrum smoothness. The grades of the lip and philtrum are dependent upon race, age, and population mean. View and download the Diagnostic Tools to learn how to measure philtrum smoothness and upper lip thinness accurately.
Palpebral Fissures
The palpebral fissure length is defined by the distance between the endocanthion (en) and exocanthion (ex) landmarks. View and download the Diagnostic Tools to learn the different techniques used to measure palpebral fissures, the standards for palpebral fissure lengths, how to determine the best method, and choose the right standard.
Individuals can be diagnosed with partial FAS (PFAS) if they have the diagnostic criteria of FAS without all of the physical features (growth impairment, decreased head circumference). PFAS is uncommon.
Alcohol-related Birth Defects (ARBD)
Individuals with alcohol-related birth defects (ARBD) have problems with congenital anomalies caused by prenatal exposure to alcohol, but may not show evidence of neurocognitive or neurobehavioral problems (ND-PAE). ARBD is uncommon. ARBD is caused by the impact of prenatal exposure to alcohol on how an individual’s organs were formed and/or how they function. Some anomalies are listed below:
- Cardiac: atrial septal defects (a hole in the heart between the upper chambers (atria)), unusual large vessels, ventricular septal defects (holes in the wall that separates the lower chambers (ventricles) of the heart), and/or other congenital cardiovascular anomalies conotruncal heart defects, and/or cardiac defects
- Skeletal: radioulnar synostosis, vertebral segmentation issues, large joint contractures, scoliosis
- Renal: aplastic, hypoplastic, or dysplastic kidneys; “horseshoe” kidneys; and/or ureteral duplications
- Eyes: Extra folds, strabismus (crossed eyes), ptosis (drooping eyelids), retinal vascular anomalies, and/or optic nerve hypoplasia
- Ears: “Railroad track” ears, conductive or neurosensory hearing loss
Additonal Resources
Last Updated
01/30/2025
Source
American Academy of Pediatrics