Although the term failure to thrive is common, inadequate growth is more accurately termed undernutrition or malnutrition.
Children with mild to moderate malnutrition have a 2.2-fold greater chance of mortality. (ref)
Children in upper/middle- and high-income countries have mal- or undernutrition for various reasons
- Chronic disease: Prevalence associated with subacute or chronic illness ranges from 6% to 32%.
- Inflammation, acute or chronic.
- Parental socio-emotional and behavioral issues.
- Depression, stress, marital strife, divorce, substance use
- Parental history of abuse as a child
- Young and single parents without social supports
- Social isolation or poverty
- Parents overly focused on career or activities away from home
- Lack of knowledge of normal growth and development
Newborns, infants, and children who fall below weight-for-age or weight-for-length percentile or whose rate of weight gain declines across 2 major percentiles (ie, 90th, 75th, 25th) should be assessed for undernutrition.
- Percentiles of weight for age or weight for length may or may not indicate abnormal growth depending on clinical circumstances.
- Undernutrition is more likely in newborns, infants, and children with abnormal patterns of weight gain over time, although some newborns, infants, and children with adequate nutrition fall into the extreme tails of standard distributions.
- Z scores (standard deviations from the mean) are the most accurate way to assess nutritional status.
- Mid-upper arm circumference (MUAC) is a good proxy for weight and a powerful indicator of mortality in children between the ages of younger than 6 months and 5 years.
- It is particularly helpful in hospitalized children who are critically ill.
- MUAC is an accurate nutritional assessment in patients with fluid shifts and edema.
- There are no reference standards for MUAC in infants <6 months
Definitions and Diagnostic Criteria
Severe acute malnutrition (SAM): weight for height (or length) that is less than –3 SDs from the mean or a mid- to upper-arm circumference between 11.5 and 12.5 cm
Moderate acute malnutrition: weight for height (or length) that is between –2 SDs and –3 SDs from the mean or a mid- to upper-arm circumference <11.5 cm
Underweight: a weight-for-height z score that is less than –2 SDs; also called wasting
Stunting: height-for-age z score more than –2 SDs from the mean
Short stature: height for age less than –2 SDs; if occurring without wasting is not malnutrition
Statistics derived from the National Health and Nutrition Examination Survey (2004–2014) show that undernutrition is common in the United States.
- The rate of mild to moderate undernutrition in females is 20.3%; in males, 21.7%.
- The rate of severe undernutrition in males and females is 4.1% to 4.2%.
- Undernutrition was found across all race, ethnicity, and income categories.
- A considerable proportion of children meet the criterion of undernutrition up through age 13 years.
Diagnostic Criteria (Z-Scores) for Undernutrition
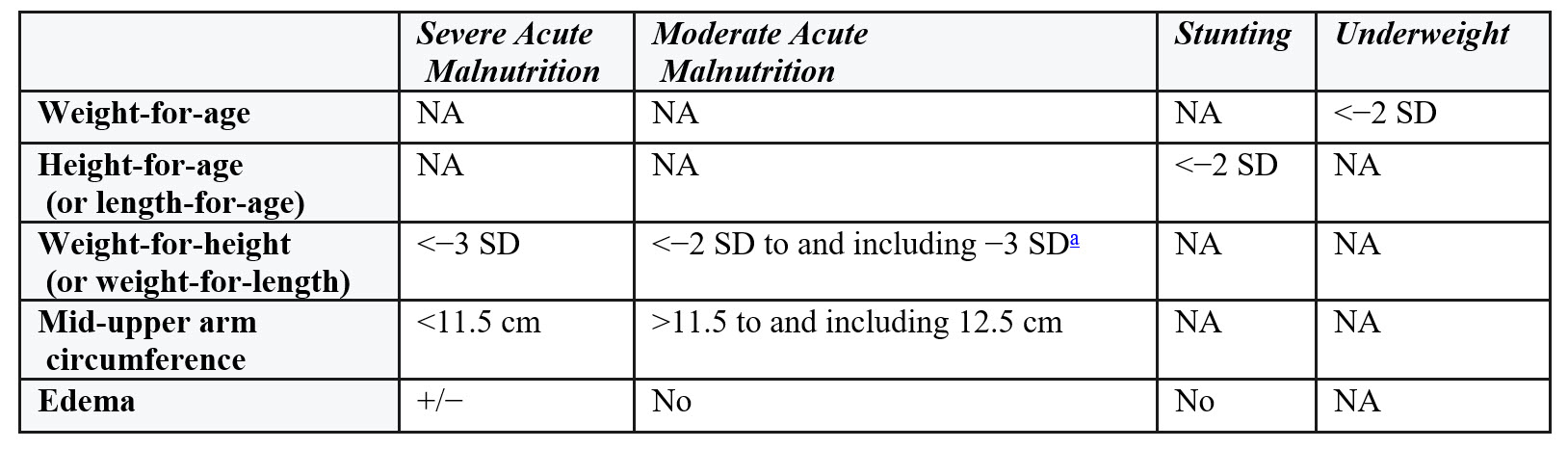 a Weight for height of <−2 SD is defined as wasting with severe wasting as <−3 SD.
a Weight for height of <−2 SD is defined as wasting with severe wasting as <−3 SD.
Evaluation
Undernutrition can result from increased energy needs, inadequate energy supply, or a combination of these.
- Any infant or child with undernutrition should be promptly evaluated.
- A thorough history and physical examination directs further evaluation.
- Keep in mind conditions that require increased energy and those that result in a deficient energy supply.
- Laboratory testing tends to be negative and unhelpful when evaluating undernutrition, except in the absence of historical or physical evidence of an underlying condition.
- Feeding, observation, and monitoring for weight gain is the first evaluative step.
Conditions requiring increased energy utilization include
- Chronic heart disease (congenital or acquired)
- Chronic lung disease
- Chronic anemia
- Chronic infection
- Endocrine abnormalities
- Malignancy
- Chronic renal disease
- Hepatic insufficiency
- Metabolic disease
- Disorders of amino acid or carbohydrate metabolism
- Idiopathic hypercalcemia of infancy
- Hormonal disturbances
- Genetic conditions
- Down syndrome
- Cornelia de Lange syndrome
- Cri du chat syndrome
- Smith-Lemli-Opitz syndrome
- Familial dysautonomia
- Micronutrient deficiencies
- Iron
- Zinc
- Carnitine
Conditions that result in deficient energy supply include
- Calories withheld
- In utero conditions
- Formula preparation mistakes
- Breastfeeding difficulties
- Parent-child psychosocial dysfunction
- Maternal depression
- Intentional abuse or neglect
- Poverty
- Unsound parental beliefs regarding nutrition
- Feeding difficulties
- Calories not properly ingested or digested
- Oral pain
- Anorexia
- Reflux esophagitis
- Emotional deprivation
- Chronic infection
- Dysphagia
- Structural abnormalities of the oropharynx or nasopharynx
- Cleft palate
- Choanal atresia
- Treacher Collins syndrome
- Pierre Robin sequence
- Laryngeal web
- Structural abnormalities of the gastrointestinal tract
- Stenosis or atresia
In addition to a thorough history and physical examination, observing a feeding can be informative. This is critical in infants who are breastfed.
In the absence of evidence of an organic condition that may lead to malnutrition, the yield of a laboratory investigation is low.
- Testing for malabsorption, endocrine disorders, occult infection, malignancy, and cardiac, pulmonary, or renal abnormalities should be done only in the presence of historical or physical examination evidence of these diagnoses.
Treatment
An algorithm for addressing malnutrition guides its treatment.
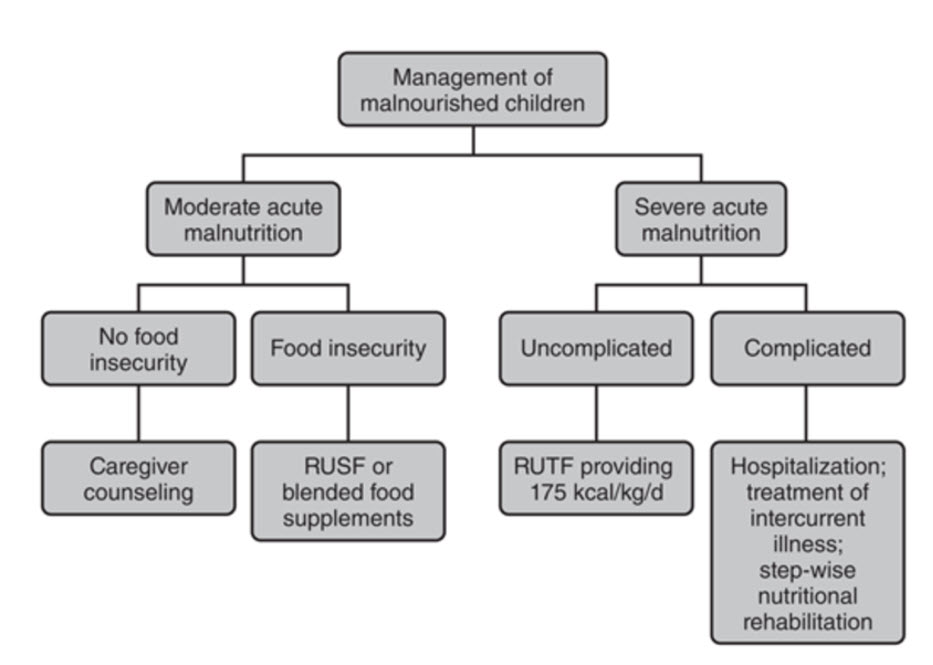
RUSF – ready to use supplementary food
RUTF – ready to use therapeutic food
Treating Moderate Acute Malnutrition
- Focus on nutritional rehabilitation, parental education, and behavioral intervention.
- Avoid overfeeding malnourished newborns and infants at the outset of therapy because refeeding that is too vigorous may induce malabsorption and diarrhea.
- The refeeding regimen should be calculated to provide about 10% to 15% of calories from protein, 50% to 60% from carbohydrate, and 30% to 40% from fat.
Refeeding occurs in phases.
Phase 1: Provide 100% of daily age-adjusted energy and protein requirements based on the newborn’s or infant’s weight on day 1. Equally important is engaging the parents in an educational program that focuses on family interactions, psychological vulnerabilities, and social needs. Emphasis should be on appropriate nutritional information.
Phase 2: If phase 1 is well tolerated, increase intake to provide adequate nutrition to achieve catch-up growth. Multiplying the age-adjusted energy requirements (kcal/kg/d) by the ratio of the newborn’s or infant’s ideal body weight for height divided by their actual body weight at presentation generates a reasonable estimate. Usually the energy and protein requirements can be accomplished with the use of a routine infant formula modified to increase its caloric density.
- For example, mix 13 oz of concentrated formula with 10 oz of water rather than 13 oz of water to create a formula that is 24 cal/oz.
- Alternatively, use carbohydrates (glucose polymers) or fat (medium-chain triglycerides) to add calories while avoiding the complications of overhydration.
- Formula may be added to expressed human (breast) milk (as an alternative to using concentrated formula) to increase caloric density,
Phase 3: Offer nutrition ad libitum as the newborn or infant gradually approaches ideal body weight. Multivitamin and iron supplementation should be part of every refeeding regimen for newborns and infants who are undernourished.
Sample Rehabilitation Schedule for Malnutrition
Scenario: A 6-month-old boy with poor weight gain is referred for nutritional rehabilitation. He currently weighs 5.5 kg and is 67 cm in length. The 50th percentile weight for this length is 7.7 kg, putting the infant at 71% of the ideal body weight for height.
Normal adjustment catch-up requirements include the following:

Treating Severe Acute Malnutrition
Children with SAM are divided into 2 groups for treatment purposes.
- Uncomplicated SAM
- Is defined by the presence of a good appetite and the absence of general danger signs or medical conditions requiring hospital admission.
- The absence of edema.
- Generally managed in the outpatient setting.
- The World Health Organization recommends treating all cases of SAM with routine antibiotics.
- Complicated SAM
- Children with complicated SAM require hospital treatment.
- Often the reason caregivers seek medical help is not the malnutrition but an intercurrent illness.
- Malnutrition markedly increases the risk of mortality secondary to the intercurrent illness (eg, pneumonia, gastroenteritis), and that risk is closely related to the severity of the wasting.
- Mortality rates of 10% to >20% have been reported for hospitalized children with SAM, with mortality being the highest in children younger than 2 years. [ref][ref]
- Treatment of infections with antibiotics and nutritional rehabilitation are the central elements of hospital-based management of SAM.
Refeeding syndrome is a metabolic shift in phosphate, potassium, and magnesium that occurs when a child converts to a fed state.
- Refeeding syndrome can have serious and life-threatening results.
- The safest approach is to monitor electrolytes, including phosphorus, potassium, and magnesium frequently.
Management
Once identified, poor weight gain in infancy should be followed up assiduously.
- Initially, weekly visits for newborns and infants may be necessary.
- Hospitalized infants younger than 6 months, when provided with adequate calories, begin to gain weight in a few days.
- Older infants and children may take longer than their younger counterparts before sustained weight gain is established.
- Ongoing developmental, behavioral, and social evaluations must be incorporated into any plan for follow-up.
When to Refer
- Diagnosis or suspicion of a chronic disease.
- Psychosocial family dynamic that indicates a need for psychiatric intervention for either or both parents.
- Nutritional rehabilitation that warrants the attention of a nutritionist.
- Suspicion of intentional nutrient deprivation or neglect requires a referral to child protective services.
![]()
The development of this resource was made possible with support from Abbott. The AAP maintains full independence in its editorial and strategic activities. Financial supporters have no influence over AAP content, policies, or leadership decisions.
Last Updated
02/13/2026
Source
American Academy of Pediatrics