A foundation of these resources is the importance of nutrition advocacy. Nutrition is critical to the healthy growth and development of young children. Pediatric professionals can drive healthy results through nutrition advocacy, which involves educating themselves, families, communities, and peers about nutrition and nutrition-related topics.
The Importance of Pediatric Professionals in Nutrition Advocacy
Pediatricians and other pediatric professionals have a critical role in promoting healthy nutrition, due to their expertise and the trust they have with families and communities.
A pediatrician exerts influence in several ways.
- Family: The physician understands each family’s needs and communicates with caregivers to offer anticipatory guidance and supportive information.
- Community: Pediatricians are expert resources and advocates within communities, in collaboration with schools and child care providers, among others.
- Peers: Pediatricians work with other pediatric specialist physicians. They also work within their own practices and peer groups guiding, supporting, and receiving guidance.
The trust that parents place in pediatricians is evident.
>80% of parents regard pediatricians as their chief source of advice for their child’s emotional and physical well-being. (ref) This national survey conducted by Stanford University in 2023 also showed that
- 88% of parents said they trust their pediatrician overall.
- 64% said they were more likely to sign up for federally based food assistance if their pediatrician told them they were eligible.
Pediatricians continuously strive to improve practice by improving their skills and knowledge and working to advocate for children in their spheres of influence—with patients and families, their communities, and among their peers.
Promoting Healthy Nutrition in Practice
Engaging in nutrition advocacy involves several factors. To effectively promote healthy nutrition, and address and prevent the long-term negative effects of poor nutrition, physicians should engage in
- Personal education: These endeavors include CME, latest research, and most current recommendations regarding nutrition-related interventions and screening.
- Community advocacy: The child and family exist within a community that affects their nutritional status and choices.
- Peer-to-peer support: Pediatricians can benefit from the support and advice offered by their peers’ knowledge, shared challenges, and plans for implementing changes in practice.
Personal Education
Implementing guidelines and recommendations in practice is not straightforward. A physician must be knowledgeable in multiple aspects of nutrition and skilled in organizing and effectively relaying that information.
Providing guidance to families means balancing issues of food security, food safety, and health effects with a specific family’s needs, expectations, and ability to follow a particular dietary pattern.
Enablers to implementing nutrition guidance include
- Knowledge
- Guidelines and recommendations
- Barriers and facilitators to implementation
- Clinical supports
- Decision support tools
- Family education materials
- Understanding the role of the community and the social drivers of health (SDOH)
- Communication skills
- Creating a supportive environment in the medical home
Nutrition Knowledge: Guidelines, Barriers, and Facilitators
In the United States, child malnutrition (both under- and overnutrition) is a pervasive issue affecting long-term health and well-being.
- Barriers to appropriate nutrition care may include
- The lack of a single undernutrition screening and assessment method
- Limited clinician awareness of nutritional issues
- Lack of education in nutrition
- Perceived difficulty in changing patient behaviors
- Inability to effectively address SDOH
Undernutrition
Measuring height and weight is critical in assessing and screening children for malnutrition. Childhood undernutrition occurs in the United States
- Often as a result of acute or chronic conditions and their treatments
- As a result of SDOH
- Food insecurity that can include imbalances in a child’s intake of energy or nutrients, including deficiencies
Undernutrition is underdiagnosed in both acute care and ambulatory settings
- Consensus guidelines from the Academy of Nutrition and Dietetics and the American Society for Parenteral and Enteral Nutrition suggest a standardized set of diagnostic indicators for use in acute care, residential settings, and ambulatory care.
- Z scores for weight-for-height/length, body mass index-for-age, or length/height-for-age or mid-upper arm circumference
- When 2 or more data points are available, indicators may also include
- Weight gain velocity (<2 years of age)
- Weight loss (2–20 years of age)
- Deceleration in weight for length/height z score
- Inadequate nutrient intake
Barriers to screening for food insecurity in primary care include
- Limited financial resources, time, incentives, and payment
- Limited knowledge about food insecurity and its prevalence
- Complexities regarding referral to services and limited resources to address food insecurity
- Concerns about privacy and stigma
Approximately 80% of pediatricians reported willingness to screen for food insecurity, but far fewer 15% (as of 2017) implemented screening.
- The greatest concern was lack of knowledge of how to handle positive screen results.
Facilitators to food insecurity screening and interventions in primary care settings include
- Trust between staff and patients
- Most families are open to revealing food security concerns in the pediatric clinic setting.
- In one 2020 study, most families agreed that they would be comfortable telling the truth (78.3%) and would feel better understood (67.9%) when screened for food security.
- Patients preferred having a nurse ask the screening questions (41.2%).
- Multiple screening modalities (self or staff-administered)
- Assistance navigating community resources.
- The most popular intervention preference was receiving a list of food bank locations (76.4%) and local community organizations (71.6%) and to have referral to financial assistance programs (75.4%). (ref)
Assessing and Treating Overnutrition in Primary Care
Obesity is one of the most common chronic diseases of childhood.
- Approximately 14.4 million children are affected.
- The effect of obesity escalates over time and early identification and treatment are recommended.
Effective primary care obesity treatment depends on health risk assessments and patient-centered counseling
- These 2 activities are positively predicted by
- Relevant training
- Belief that pediatricians play an important role in obesity
- Awareness of barriers to payment for dietitians or weight management programs
- These activities were negatively predicted by
- Perceived lack of available primary care pediatrician time
- Inadequacy of available referral resources
- Belief that patients and families lack time for healthy behaviors
Implementing nutrition guidelines varies according to setting and topic.
- Pediatricians in hospital/clinic settings reported discussing healthy behaviors less than group or solo/2-physician practices.
- A 2020 survey showed that
- ~80% of pediatricians use the World Health Organization growth charts at all well visits.
- Nearly half (45.3%) recommend solid food introduction at 6 months.
- However, slightly more (48.2%) recommend <6 months.
- Cereals are more frequently recommended at <6 months than fruits/vegetables or meats.
- However, slightly more (48.2%) recommend <6 months.
- Topics most frequently discussed were
- Limiting juice (92.3%)
- Limiting sugar-sweetened beverages (92.0%)
- Least discussed topics are
- Avoiding restrictive and permissive food practices (30.7%)
- Avoiding food as a reward (29.1%)
Clinical Supports
Nutrition implementation guidance for pediatric practice
Undernutrition
Assessing undernutrition in the inpatient setting
- A voluntary measure in the Pediatric Quality Measures Program offers hospital-based nutrition screening guidance.
- The guidance asserts that “an initial baseline screen of nutritional status for every PICU patient increases awareness of his/her nutritional state, identifies patients at risk for malnutrition, and allows providers to adjust the timing, content, and quality of nutrition therapy to meet the individual patient’s needs.”
Assessing undernutrition in the ambulatory setting
- The AAP recommends pediatricians implement universal screening for food insecurity.
- Resources are available from the AAP for implementing this recommendation.
- Federal and local resources for food support.
- Ensure families avoid limiting their purchases of produce or other plant foods that are not organic, believing that “regular” produce is harmful. Furthermore, promoting organic food may cause unnecessary stress for families who are struggling financially.
- The AAP provides resources to assist pediatricians in encouraging healthy, active living, which includes advice on nutrition and exercise (with a focus on establishing healthy lifestyles in early childhood).
Overnutrition: Encouraging Appropriate Nutrition Habits
- The AAP published a clinical practice guideline on obesity diagnosis and treatment.
- Supporting materials include an algorithm, summary recommendations, and key action statements.
- The AAP Institute for Healthy Childhood Weight provides myriad resources for physician continuing education, quality improvement activities and patient resources.
- The AAP provides resources to assist pediatricians in encouraging healthy, active living, which includes advice on nutrition and exercise with a focus on establishing healthy lifestyles in early childhood.
- The AAP provides a PediaLink module that educations young physicians on supporting breastfeeding in the practice setting.
- Other breastfeeding support materials for physicians and mothers
General Nutrition Implementation Guidance
When speaking with parents, pediatricians should focus on the following evidence-based points:
- Use motivational interviewing techniques to tailor guidance and advocate for optimal nutrition.
- Screen for food insecurity at all visits.
- Help parents identify the attributes of nutrient-dense foods (rich in essential vitamins, minerals, protein, fats, and fiber relative to the number of calories).
- Key recommendations for toddler and preschool-aged children
- Consume adequate potassium, fiber, vitamins D and E, iron, and calcium.
- Choose nutrient-dense foods.
- Encourage vegetables, fruits, whole grains, and iron- and zinc-rich animal source foods.
- Encourage consumption of water and lowfat dairy or alternatives fortified with calcium and vitamin D.
- Limit sodium, added sugars, and saturated fat.
- Limit 100% juice consumption.
- Avoid energy-dense, nutrient-poor snacks.
- Avoid sugar-sweetened beverages, flavored milks, affeinated beverages and beverages with low-calorie sweeteners. Avoid formulas designed for older children unless medically indicated.
- Encourage a structure in the home that limits access to sugary and processed foods while providing nutrient-dense options.
- Offer repeated exposure to new nutrient-dense foods.
- Have family meals as often as possible.
- Limit eating out or take-out foods.
- Limit the amount of sugary or highly processed foods in the home.
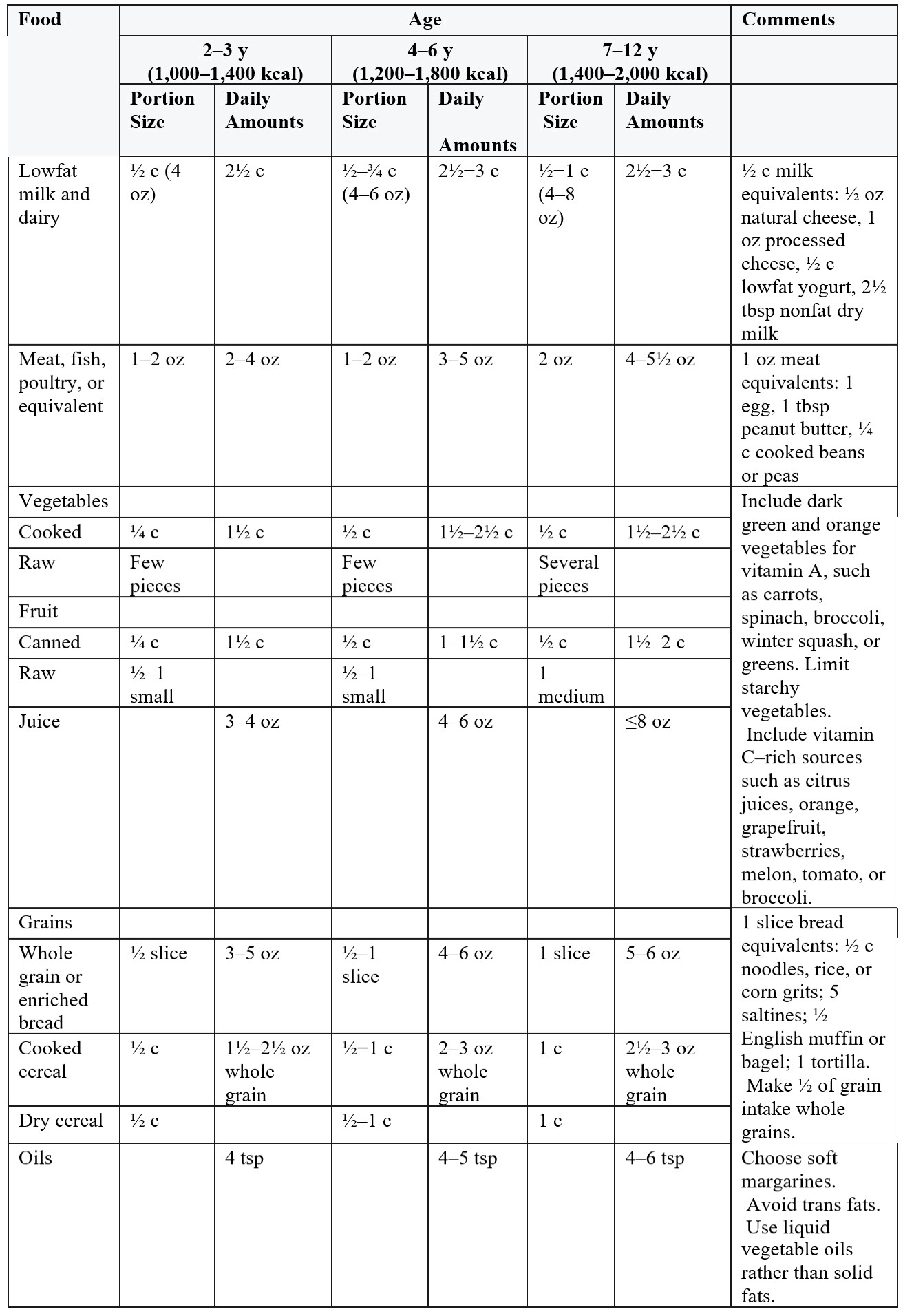
- Use child portion sizes (see Feeding Guide).
- For children 2 to 6 years of age, initially offer 1 tablespoon for every year of age, with more provided according to appetite.
- Offer healthy options at planned snacks and meals.
- Encourage child autonomy.
- Model healthy nutritional behaviors.
- Praise children for making healthy choices.
- Avoid coercive and controlling practices.
- Offer fixed choice between healthy options.
- Be responsive to child hunger and satiety cues.
Healthy portion sizes may not be obvious to parents, particularly those who are new parents or who themselves struggle with portion size.
- Consider making the following feeding guide available for parents.
- Encourage healthy finger foods for infants and toddlers with this poster showing food preparation tips for young eaters.
Feeding Guide
Communication Skills
Communicating openly and with compassion is essential for effective and efficient routine health care.
- Health care communication is critical but is often absent or minimal in curricular materials for physicians and other health care professionals.
- Learning communication skills involves practice, feedback, and mentoring.
Resources for learning and teaching effective communication
- The AAP provides information on strength-based approaches, motivational interviewing, and plain language.
- The Academy of Communication in Healthcare provides web-based, multimedia interactive modules on communication and relational topics.
- The Maryland Chapter of the AAP quality improvement project has developed materials to support motivational interviewing techniques and essential communication skills.
Healthy Nutrition in the Community
Improving the health of children means promoting healthy communities and understanding the SDOH. SDOs are nonmedical conditions that can affect nutritional status and, thus, overall health. The most well-known SDOH affecting nutritional status is socioeconomic status.
Other SDOHs that affect nutrition are
- Employment status.
- Immigration status.
- Refugee status.
- Disability.
- Limited access to grocery stores.
- Lack of transportation.
- Lower education levels.
- In the United States, children in urban areas have a higher prevalence of food insecurity compared to their rural counterparts.
As part of the US Healthy People 2030 goals, food security was identified as a SDOH.
- At the community level, nutrition security has become a heightened area of focus for clinicians leading to recommendations for universal screening.
Other ways to promote healthy nutrition in communities
- An AAP resource regarding Nutrition in Schools provides information to physicians when advocating for optimal nutrition for all children or for specific patients with special needs.
- Partnering with community members can improve the infrastructure for healthy living.
- Review other published examples of partnering with community stakeholders to promote early childhood healthy weight in a rural setting and in family child care.
- Learn about AAP advocacy efforts by signing up for legislative alerts or downloading the Digital Advocacy tool.
- Follow the legislative activities of The Food Research & Action Center.
- Become familiar with national legislative affecting school nutrition offered by the School Nutrition Association.
Peer-to-Peer Education
Pediatricians support one another in implementing nutrition recommendations by
- Providing advice and guidance
- Participating in formal speaking engagement on topics of personal expertise
- Proposing quality improvement projects to improve specific aspects of nutrition care
- Referring to and publishing articles regarding quality improvement projects
One example of a successful quality improvement project improving nutritional support for children in an office setting
- The goal: Improve Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) enrollment.
- The method: Improve screening and referrals for enrollment.
- The results: A 42% increase in WIC enrollment and an increase in provider knowledge of WIC services.
- Families reported that barriers to WIC enrollment were access problems and lack of knowledge about WIC
Pediatricians wishing to work with their peers to improve the implementation of nutrition recommendations can find information on quality improvement from the AAP.
![]()
The development of this resource was made possible with support from Abbott. The AAP maintains full independence in its editorial and strategic activities. Financial supporters have no influence over AAP content, policies, or leadership decisions.
Last Updated
02/13/2026
Source
American Academy of Pediatrics