Pediatric tobacco use and nicotine dependence are significant health concerns. Despite declines in cigarette use, youth still use tobacco products—including e-cigarettes—at high rates. Adolescents and young adults are uniquely vulnerable to nicotine dependence, and nearly 90% of adult tobacco users start before the age of 18, according to CDC data. Effective strategies to promote youth tobacco cessation are urgently needed.
The evidence base for youth tobacco cessation is limited and research is urgently needed to fill gaps in the literature. In the meantime, clinicians can leverage existing literature and promising practices to support cessation in young people.
The American Academy of Pediatrics (AAP) has a long history of addressing tobacco use among youth via education, clinical policy, public policy and advocacy. This resource is intended to support all pediatric health clinicians in helping young patients quit tobacco use. Please note that this resource does not serve as official policy of the AAP, or as a clinical guideline. Rather, this resource is designed to provide practical advice and considerations for addressing tobacco cessation in youth. For more resources on helping youth quit tobacco, nicotine products, and reduce exposure to secondhand smoke, please visit our main page.
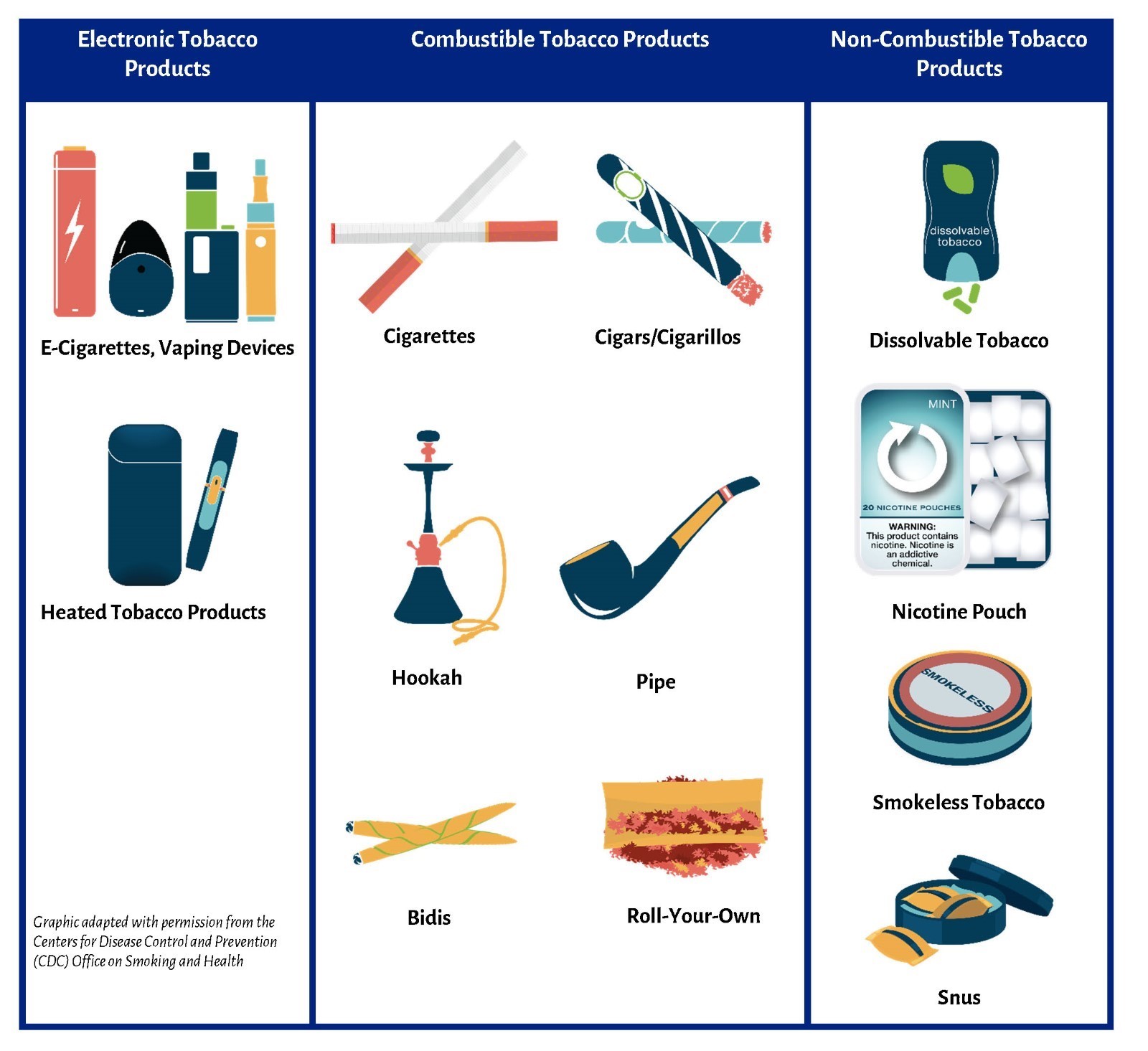
This resource is intended to support youth cessation of all commercial tobacco products, including (but not limited to) those below:
Ask-Counsel-Treat (ACT) Model for Youth Cessation
Minimize time and burden on the pediatric health clinician and maximize the patient’s chances of a successful quit. Pediatric health clinicians have a collective responsibility to ACT to identify youth who use tobacco and connect them with the resources they need for a successful quit.
Ask
Screen for tobacco use with all youth, during every clinical encounter.
Counsel
Advise all youth who use tobacco to quit and have them set a quit date within two weeks.
Treat
Link youth to behavioral treatment extenders and prescribe pharmacologic support when indicated. After the visit, follow-up to assess progress and offer support.
Printable A.C.T. Model Flowchart Considerations for Clinicians PDF
Last Updated
05/19/2025
Source
American Academy of Pediatrics