Carrie Daymont, Faerber Jennifer, Chris Penney, Alexander Fiks, Ian Paul, Wenke Hwang, Hadassah Polydore, Chelsea Emrick, Teniel Badriaki, Brennen Harding, Allison Hess, Teresa Rivas, Katherine Ruggiero, Emily Simone, Eric Schaefer
Presented at the 2026 Pediatric Academic Societies Annual Meeting
Background: Measurement and recording errors in weight (WT) and length or height (HT) can affect clinical decisions and can also impact research analyses and study conclusions, even after data cleaning.
Objective: To evaluate the impact of varying types and degrees of WT and HT errors on the apparent prevalence of obesity.
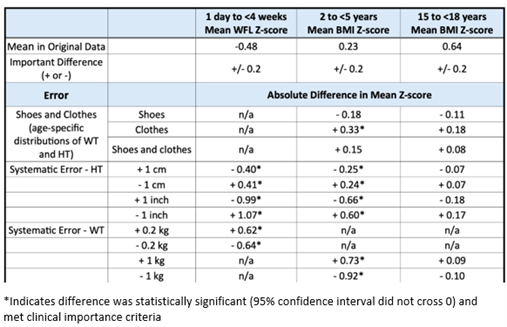
Methods: We evaluated data from 2 research networks separately in secure environments. After cleaning the data with a validated algorithm, we identified children with a WT and HT measurement on the same day in 2018. Within each network, we randomly selected cohorts of 2000 children in 10 age groups and randomly selected one measurement set for each child. The primary outcome was the proportion of children in each cohort with obesity: ≥95th percentile for weight-for-length (WFL, < 2 years) or body mass index-for-age (BMI, ≥2 years). Incorporating stakeholder input, we identified types and degrees of WT and HT error to evaluate. For each error, we altered the original data to imitate the error, creating “error data”. For example, for the “clothes” error, the error data contained a variable amount added to each WT measurement to imitate children wearing different types of clothes. For one error/age group combination at a time, we determined the differences in the prevalence of obesity in the original data compared to the error data, obtaining confidence intervals for these differences using bootstrapping. Based on expert opinion, we defined a clinically important difference in prevalence as a relative difference of +/-10% of the prevalence in the original data (minimum +/- 1%). We also evaluated differences in mean WFL or BMI z-score (clinically important difference +/- 0.2).
Results: In infants and young children, the differences in obesity prevalence and mean z-score often met clinical importance criteria, even for small errors (Tables). In older children and adolescents, some larger errors resulted in clinically important differences in obesity prevalence. Adding WT to imitate clothes resulted in a higher mean BMI. When imitating shoes, the average impact of added HT was larger than that of added WT, resulting in a lower mean BMI. Results from both networks were similar.
Conclusion: HT and WT errors of a magnitude seen in real-world conditions can cause clinically important differences in the apparent prevalence of obesity. Clinicians must be aware of the potential impact of common degrees of error when they base decisions on WFL and BMI. Variable data quality could lead to between-center variability in apparent obesity prevalence, which should be considered when making comparisons.
Table 1. Differences in apparent prevalence of obesity with selected errors from one network.
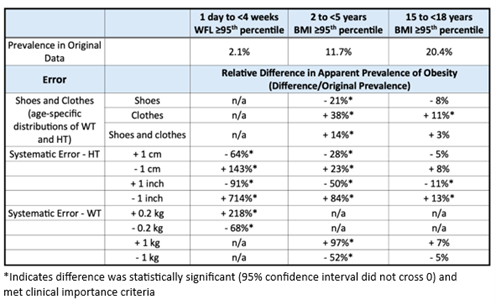
Table 2. Differences in mean z-score with selected errors from one network.
Last Updated
05/05/2026
Source
American Academy of Pediatrics