Alexander Fiks, Yun Li, Mary Kate Kelly, Ziyi Wang, Julia Szymczak, Jennifer Steffes, Kristin Davis, Donna Harris, Nicole Hackman, David Kaelber, Matthew Tien, Dane Snyder, Keith Portillo, Sharon Humiston, Nicholas Riley, Brandi Muller, Everly Macario, Robert Grundmeier, Jeffrey Gerber
Presented at the 2026 Pediatric Academic Societies Annual Meeting
Background: Although antibiotics can be lifesaving drugs, up to half of all antibiotic use is inappropriate.
Objective: To measure the effectiveness of an evidence-based, outpatient antibiotic stewardship intervention for children with acute respiratory tract infections (ARTI) when scaled across health systems.
Methods: From 2021-24, we conducted a clinician-level, cluster RCT to improve ambulatory ARTI antibiotic prescribing in children 6 months to 12 years-old across 5 health systems with 139 primary care, 10 urgent care, and 16 emergency department sites. The intervention (compared with usual care) included 3 online educational modules detailing appropriate ARTI prescribing; 4 feedback reports of individual prescribing performance with peer comparison; and local site champions. Primary outcomes were: (1) the proportion of encounters for bacterial ARTI during which a broad-spectrum antibiotic was prescribed; (2) the proportion of visits for all ARTI (viral and bacterial) during which an antibiotic was prescribed; and (3) engagement, measured as number of educational modules and feedback reports viewed. We applied generalized linear mixed-effects logistic regression models to compare 1-year baseline with 1-year post-intervention periods.
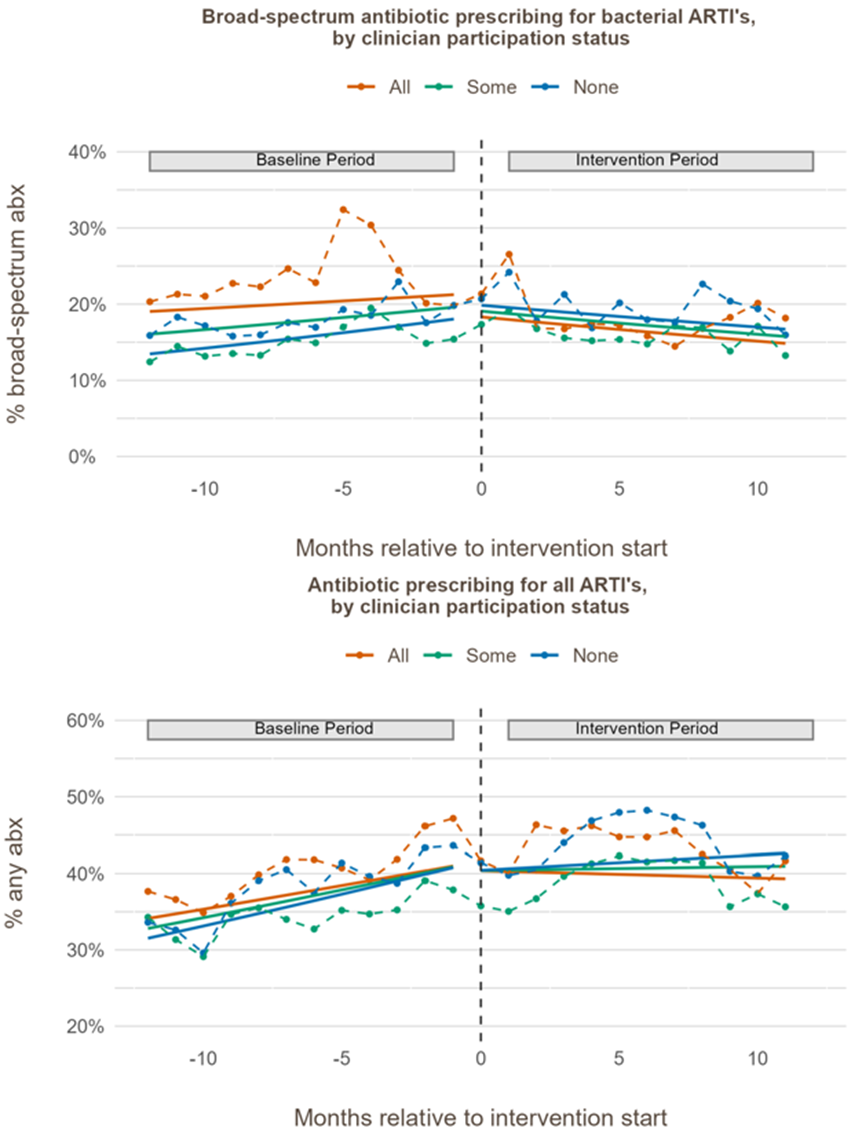
Results: Table 1 shows visit level characteristics. For bacterial infections, the monthly rate (slope difference) of broad-spectrum antibiotic prescribing declined faster in the intervention group than in the control group but did not differ significantly between groups (OR=0.985; 95% CI: 0.970–1.001) (Figure 1). For all ARTIs, the monthly rate of decline in prescribing any antibiotic was also faster in the intervention group versus control group, but the difference was not statistically significant (OR=0.992; 95% CI: 0.980–1.004). Overall, 14% of clinicians engaged with all 7 educational modules and feedback reports, 45% with some, and 41% with none. When clinician engagement was included as a covariate in the regression models, higher activity completion was associated with a greater reduction in broad-spectrum antibiotic prescribing (OR=0.920 for each additional activity completed; 95% CI: 0.904-0.936) and overall prescribing rates (OR=0.977; 95% CI: 0.964–0.990) (Figure 2).
Conclusion: Scaling an evidence-based intervention across 5 health systems did not result in improved outcomes overall but was associated with improved antibiotic prescribing among those who engaged. Strategies to promote clinician engagement may be needed to maximize benefit.
Table 1. Distribution of visit-level characteristics during the baseline and intervention periods, stratified by control and intervention groups (N = # of visits)
All variables are presented as recorded in the electronic health record.
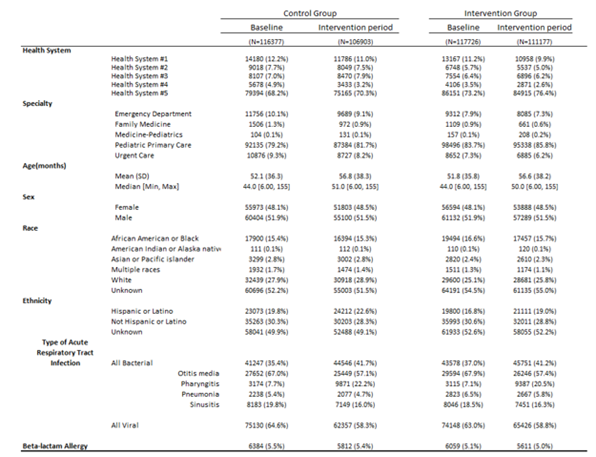
Figure 1. Trends in Antibiotic Prescribing Over Time in Control vs Intervention Groups
Monthly percentage of visits with (top) broad-spectrum antibiotic prescribing and (bottom) any antibiotic prescribing, comparing control (orange) and intervention (green) clinics. Vertical dashed line indicates the start of the intervention; solid lines show fitted trend lines.
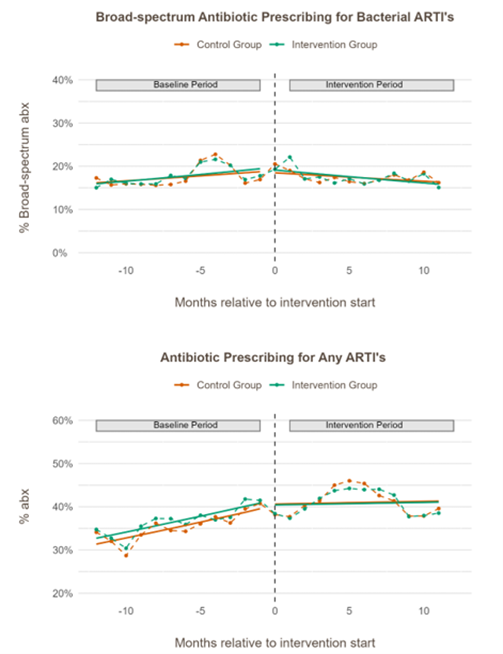
Figure 2. Antibiotic Prescribing Trends by Clinician Participation Status
Monthly percentage of visits with (top) broad-spectrum antibiotic prescribing and (bottom) any antibiotic prescribing, stratified by the degree of clinicians’ compliance with the intervention (completed all 7 activities (3 educational modules and 4 feedback reports), completed some activities, completed none). Vertical dashed line indicates intervention start; solid lines show fitted trend lines.
Last Updated
05/05/2026
Source
American Academy of Pediatrics