Mary Kate Kelly, Alexander Fiks, Samuel Wittman, Janani Ramachandran, Kristin Davis, Jennifer Steffes, Donna Harris, Everly Macario, Matthew Jones, Brigit Hatch, Julia Szymczak, Jonathan Yabes, Robert Grundmeier, Kristin Ray
Presented at the 2026 Pediatric Academic Societies Annual Meeting
Background: Asthma is one of the most common chronic conditions in children. Telemedicine (TM) visits may enhance families’ ability to attend primary care visits, discuss asthma symptoms, and titrate medications. How primary care practices are incorporating TM into their care of children with asthma and its impact are not known.
Objective: To assess whether in 2023-24 practice-level TM use for asthma primary care was associated with 2 quality metrics: documentation of asthma severity and, among those with persistent asthma, controller medication prescribing.
Methods: We retrospectively analyzed electronic health record data for children 2-18 years who received primary care for asthma at 829 community health centers, 76 practices from 2 regional health systems, and 46 independent practices from the American Academy of Pediatrics national Pediatric Research in Offices Settings (PROS) network. Using data from 2016-24, we evaluated children who had 2 or more primary care visits at least 6 months apart with an asthma diagnosis (ICD-10 J45), with at least one visit during 2023-24. We defined TM use at the practice level as the rate of TM use at asthma visits per 100 patients. We then grouped together practices that fell at or above the third quartile of TM use (high TM), those that used some TM, but fell below the third quartile (low TM), and those that used no TM for asthma. The outcomes we evaluated were asthma severity documentation (based on ICD-10 codes) and asthma controller medication use (any prescriptions during the study period for those with persistent asthma). To evaluate the relationship between TM use category (no, low, or high TM use) and these outcomes, we used mixed effects logistic regression with practice as a random effect and controlling for the fixed effects shown in Table 1.
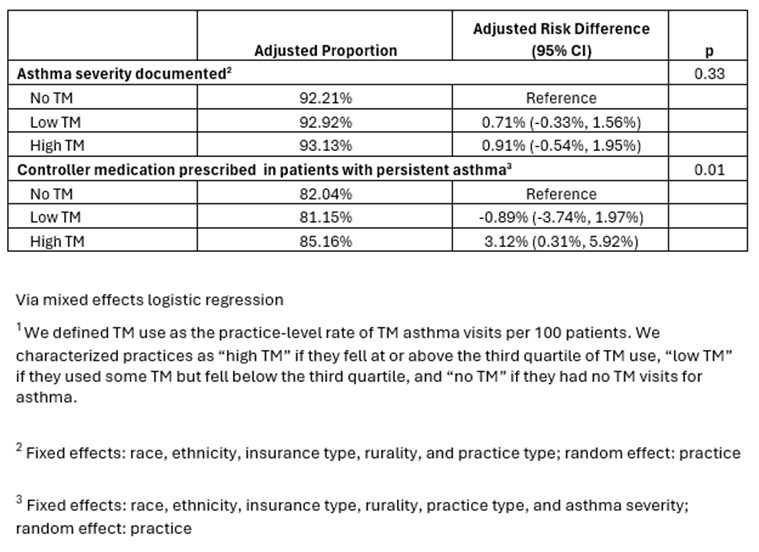
Results: Our sample included 95,123 children with asthma: 23% were seen at high TM practices, 60% at low TM practices, and 17% at no TM practices. Practice-level TM use was not associated with asthma severity documentation. However, high practice-level TM use was significantly associated with asthma controller medication prescribing. Compared to practices that did not use TM for asthma care, high TM practices had a 3.1 percentage point greater rate of children with persistent asthma with a controller prescription [95% CI 0.31%, 5.92%) (Table 2).
Conclusion: Primary care practices with higher TM use were more likely to prescribe controller medications to children with persistent asthma. Our results suggest that TM integrated into primary care practice may support evidence-based asthma care.
Table 1. Characteristics of Children Receiving Primary Care for Asthma in 2023-2024, by Practice-Level Telemedicine (TM)1 Use
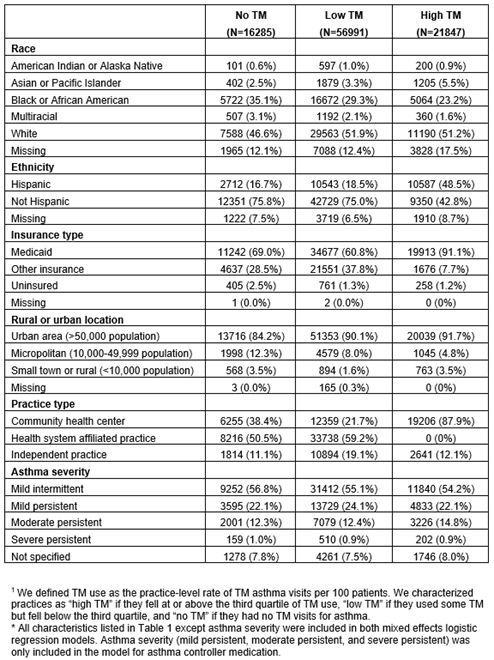
Table 2. Asthma Outcomes by Child Primary Care Site Telemedicine (TM)1 Use
Last Updated
05/05/2026
Source
American Academy of Pediatrics