Garg A, Brochier A, Torres A, Tyrrell H, Ayturk M, Barahona Paz K, Drainoni M, Fiks A, Freibott C, Griffith M, Joiner T, Shone L, Macario E, Scheindlin B, Tripodis Y, Stockwell M, Serwint J
Presented at the 2024 Pediatric Academic Societies Annual Meeting
Background: In accordance with AAP recommendations, many pediatric practices implement social needs screening and referral systems. Our prior work demonstrated the efficacy of WE CARE in community health centers for increasing low-income parents’ receipt of resources. However, WE CARE’s effectiveness in diverse practices serving publicly and commercially insured children is unknown.
Objective: To assess WE CARE’s effectiveness on parents’ receipt of community-based resources for unmet social needs.
Methods: We conducted a Type 2 hybrid effectiveness-implementation stepped wedge cluster trial in pediatric practices across the U.S. Through the AAP Pediatric Research in Office Settings (PROS) and APA Continuity Research Network (CORNET) research networks, 18 practices in 14 states participated (8 urban, 6 suburban, 4 rural). Three clusters of 6 practices each participated in Usual Care, WE CARE Training, and WE CARE Intervention phases. After training, practices piloted and implemented WE CARE, which included: 1) a self-report screener for 6 social needs (childcare, food, housing, parent education, employment, utilities) and 2) clinician access to practice-generated customized Family Resource Books with referral handouts for parents. Parents of children 2 mos-10 yrs were enrolled during both Usual Care and WE CARE phases and followed-up 3-mos post-well-child visit. Self-reported data were collected Dec 2019-Sept 2023 and analyzed using generalized estimating equation models.
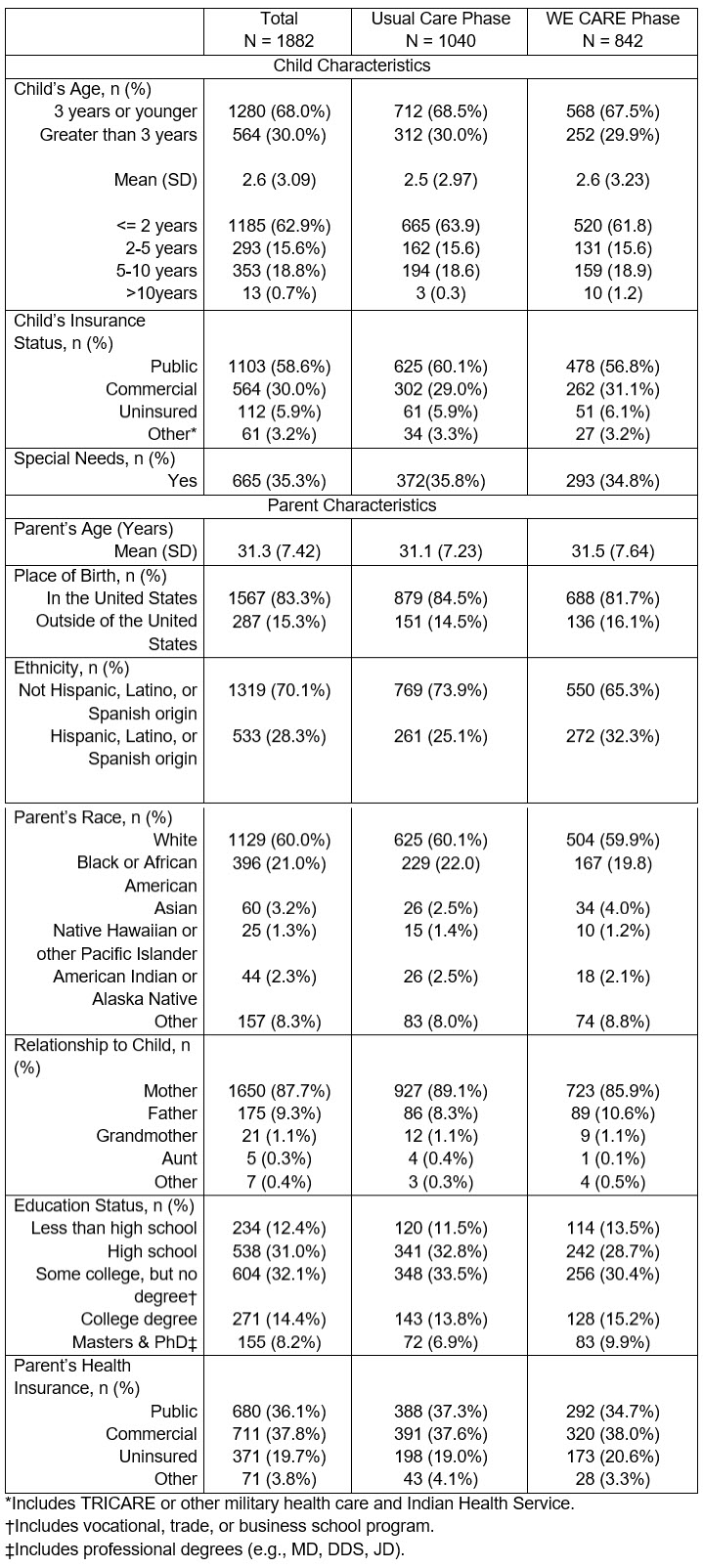
Results: 1,882 parents enrolled (WE CARE phase n=842) and 64% completed follow-up. While 59% of children were on Medicaid, 31% were commercially insured (Tab 1). More WE CARE vs. Usual Care phase parents reported discussing social needs with their child’s clinician (Tab 2) and receiving 1 or more referrals (20% vs 12%, aOR: 1.7, 95% CI, 1.3-2.2) (Tab 3). At follow-up, there were no differences between the two groups in enrollment in new resources (18% vs 18%, p=0.78). Among WE CARE parents, 60% reported having >1 social needs on screeners but only 28% received referrals.
Conclusion: Among diverse pediatric practices, WE CARE implementation was associated with higher rates of social needs discussions and referrals but no enrollment differences; however, few WE CARE parents with needs reported receiving referrals. Our results suggest that social needs screening and referral systems, as implemented in this trial during and post the COVID-19-pandemic, may have limited impact on enrollment in resources unless fidelity of the intended intervention is ensured.
Table 1. Baseline Characteristics of Participants
Last Updated
05/24/2024
Source
American Academy of Pediatrics